This is only a summary. This family or individual health insurance plan provides many outpatient services before you have met your annual medical deductible.
 Plan Names Id Card And Provider Directory Reference Guide Pdf Free Download
Plan Names Id Card And Provider Directory Reference Guide Pdf Free Download
Individual Family Plan Type.
La care silver 73 hmo. Learn more about plan monthly costpremimum deductiblesprescription drug coverage hospital services accepted doctors and more. Information about the cost of this. Is available through Covered California in Los Angeles Orange and San Diego counties and parts of Kern Riverside and San Bernardino counties.
Our Silver 70 HMO plan provides practical affordability and member out-of-pocket expenses. Silver 73 CommunityCare HMO. IndividualFamily Plan Type.
Physician office visits and urgent care before deductible. Silver 73 HMO Coverage Period. Tier 2 Preferred Brand 15.
What this Plan Covers What it Costs Coverage for. The SBC shows you how you and the plan would share the cost for covered health care services. Silver 73 HMO Bronze 60 HMO Minimum.
The 73 refers to the average percentage that the plan will generally pay for health services. Tier 4 Specialty 10 up to 250prescription. What this Plan Covers What it Costs.
Silver 73 CommunityCare HMO Coverage for. If you want more detail about your coverage and costs you can get the complete terms in the policy or plan. All Covered Members Plan Type.
What this Plan Covers What it Costs. Plan Provider You will pay the least What You Will Pay Non-Plan Provider You will pay the most. 45 85 500prescription 40 up to 0.
All Covered Members Plan Type. Molina Silver 73 HMO Coverage Period. Summary of Benefits and Coverage.
Silver 73 CommunityCare HMO. Information about the cost of this plan. Other coverage options may be available to you too including buying individual insurance coverage.
This is only a summary. Care Silver 70 HMO from LA. Health Net of CA.
Covered CA_Silver 73 HMO Coverage for. You can view the Glossary at. 01012017 12312017 Summary of Benefits and Coverage.
Care Health Plan at 1- 855-270-2327. Health Net of CA. Information about the cost of this plan.
Services You May Need. Provider network for covered beneits and services. Coverage PRESCRIPTION DRUGS Tier 1 Most Generics 5.
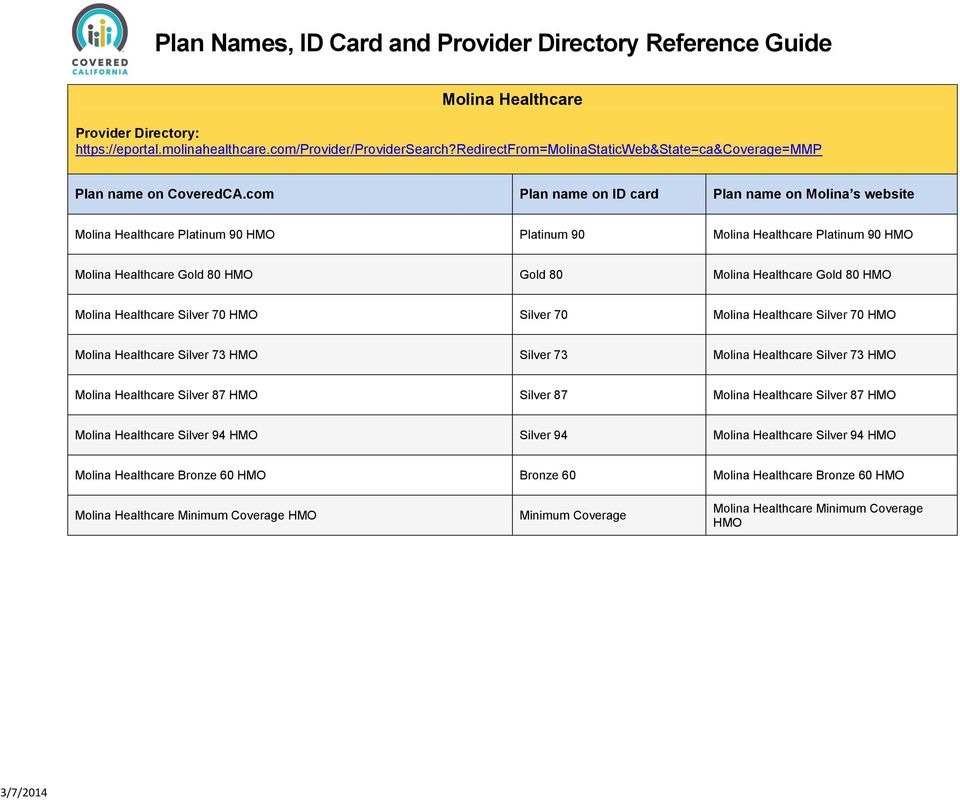
Molina Healthcare of California. Common Medical Event Services You May Need Your Cost If You Use an In-network Provider Your Cost If You Use an Out-of-network Provider Limitations Exceptions. The SBC shows you how you and the plan would share the cost for covered health care services.
Coinsurance costs shown in this chart are after your deductible has been met if a deductible applies. Silver 73 HMO The Summary of Benefits and Coverage SBC document will help you choose a health. Department of Health and Human Services at 1-877-267-2323 x61565 or wwwcciiocmsgov.
Molina Silver 73 HMO. Care at 1 888 HMO-2219 1-888-466-2219 or. The Summary of Benefits and Coverage SBC document will help you choose a health plan.
Non-Discrimination Notification Molina Healthcare. Health Net of CA. Tier 3 Non-Preferred Brand 25.
Silver 73 HMO. The SBC shows you how you and the plan would share the cost for covered health care services. What this plan covers and what it costs.
Information about the cost of this plan called the premium will be. Molina Healthcare Molina complies with all Federal civil rights laws that relate to healthcare services. Beginning on or after 01012021.
01012018 12312018 Summary of Benefits and Coverage. 25 55 500prescription 40 up to 0. For more information about your coverage or to.
All Covered Members Plan Type. 200 Oceangate Suite 100 Long Beach CA 90802. Get Health Insurance plan info on LA.
Plan called the premium will be provided separately. HMO 1 of 6 The Summary of Benefits and Coverage SBC document will help you choose a health plan. The Summary of Benefits and Coverage SBC document will help you choose a health plan.
The SBC shows you how you and the plan would share the cost for covered health care services. The Silver 73 HMO health plan utilizes the. Individual Family Plan Type.
Beginning on or after 01012019. 80 90 15. Information about the cost of this.
Beginning on or after 01012017 Summary of Benefits and Coverage. For more information about your coverage or to. Uniform Health Plan Benefits and Coverage Matrix Blue Shield of California Effective January 1 2017 THIS MATRIX IS INTENDED TO BE USED TO HELP YOU COMPARE COVERAGE BENEFITS AND IS A SUMMARY ONLY.
So under the Silver 73 enrollees may anticipate their health plan to pay about 73 of the total covered expenses. THIS MATRIX IS INTENDED TO BE USED TO HELP YOU COMPARE COVERAGE. Plan called the premium will be provided separately.
If you want more detail about your coverage and costs you can get the complete terms in the policy or plan document at. The SBC shows you how you and the plan would share the cost for covered health care services. This is only a summary.
Blue Shield Silver 73 HMO This federally subsidized plan is only available to those whose income is 200-250 above federal poverty level. Silver 73 HMO Coverage Period. This is only a summary.
Silver 73 HMO The Summary of Benefits and Coverage SBC document will help you choose a health. What You Will Pay. Generic Rx available before deductible.
Individual Family I. This plan features a deductible of 3700 per individual or 7400 for a family that is lower than the standard Silver 70 Plan.