Prior Authorization Request Form Page 1 of 2 DO NOT COPY FOR FUTURE USE. Pre-authorization fax numbers are specific to the type of authorization request.
2
1-844-403-1028 Prior Authorization Department.
Optimum authorization form. Other ways to submit a prior authorization Having difficulties with ePA. All REQUIRE MEDICAL RECORDS TO BE ATTACHED. Keep a copy of this form for your records.
PRE-CERTIFICATION REQUEST FORM. Opens a new window or tab. Part B Injectable Prior Authorization List.
The application should be completed with the assistance of a mortgage professional. Visit this section regularly to ensure you have the latest copy. This form is for pre-certification requests which will be processed as quickly as possible depending on the members health condition.
Go to Prior Authorization and Notification Tool. You may also ask us for a coverage determination by calling the member services number on the back of your ID card. Specialists should accept a PCP Electronic Medical Record EMR generated referral form as long as all Maryland Universal Referral Form fields are included.
Santa Ana CA 92799. Admissions Application Packet pdf Download. See below for a form you can complete to allow someone else to access your healthcare information or speak on your behalf.
If the Referral is mailed by the primary care physician ensure consulting physician has received his or her copy of the Referral. We are required to safeguard PHI by applicable law. I agree that I will continue to be responsible for this account including payment of all charges associated with this account and responsibility for all assets of Optimum installed at the above service address.
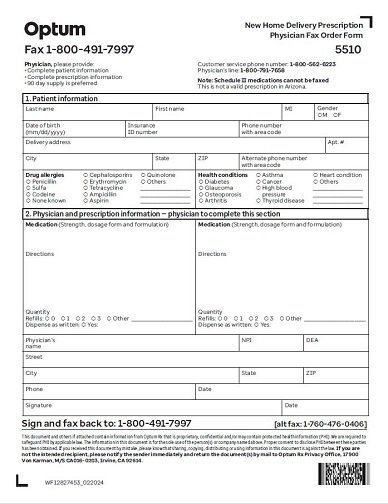
You will need a browser compatible with PDF files or you will need to download. FORMS ARE UPDATED FREQUENTLY AND MAY BE BARCODED Member Information required Provider Information required Member Name. Drug Exception Request Form.
This form may be sent to us by mail or fax. They help reduce risks to patients and improve the quality safety and appropriate use of imaging procedures. Please review your health plan covered benefits and.
A Referral is not a guarantee that the services are covered benefits. These programs support the consistent use of evidence-based professional guidelines for diagnostic imaging procedures. Prior Authorization Request Form DO NOT COPY FOR FUTURE USE.
Screening and Referral Form pdf Download. Authorize Optimum to change the name on this account as indicated on this form. Your office prescription to the form.
Do not write STAT ASAP Immediate etc. Call 1-800-711-4555 5 am. Referrals that are generated electronically using our online referral system dont need to accompany the CMS-1500 form.
Give the original Referral to yourconsultant. Release of Information ROI Authorization to Disclose Protected Health Information PHI. Prior Authorization PO Box 46770.
Standard ROIAuthorization form Spanish PDF. You can fax your requests to 1-888-992-2809 Or mail the completed form to. Physician Fax Number with Area Code Physician Street Address City State ZIP NPI.
To assist you in your mortgage process we have provided certain forms you might need along the way. Below is a list of forms used in day-to-day interactions with our Plan. Acthar Gel Nephrotic Syndrome.
Optum Standard Authorization Forms Plans administered by Optum behavioral do not require prior authorization for routine outpatient services. The referral with the CMS-1500 form to UnitedHealthcare. PT Saturday If you cannot submit requests to the OptumRx PA department through ePA or telephone click here.
866-608-9860 or 888-202-1940 Instructions. Send a secure email for Prior Authorization requests to be sent to our office. This document and others if attached contain information from OptumRx t hat is privileged confidential andor may contain protected health information PHI.
Actemra diagnosis of Giant Cell Arteritis Actemra IV Medical Actemra IV for diagnosis of Cytokine Release Syndrome CRS Medical Actemra SQ Pharmacy Non-Preferred Acthar Gel Infantile Spasms. Optum administers a wide range of benefits. Standard ROIAuthorization form English eForm.
Las Vegas NV 89114-6770. You can submit a verbal PA request. FORMS ARE UPDATED FREQUENTLY AND MAY BE BARCODED Patient Information required Provider Information required Patient Name.
Who May Make a Request. Included is obviously the Mortgage Application Form which you can download and print. Applicants download and type in the application.
Radiology Prior Authorization and Notification. PT Monday-Friday and 6 am. Prior Authorization Forms and Policies.
Please submit your request to the fax number listed on the request form with the fax coversheet.





.jpeg?width=400&height=321&name=Independent%20Physician%20Association%20(IPA).jpeg)